

This remarkable feature story summarizes the life and landmark achievements of Philip Muccio, pioneer innovator of the wearable neuromuscular rehabilitation technology for patients of traumatic brain injury and spinal cord injury. His 30+ year career in continued expansion of this science has brought regenerative relief and therapy to countless individuals worldwide and has been the launchpad to an entire industry of wearable regenerative health solutions.
The autobiography "REBUILDING THE PATH OF HOPE" is currently in its final stages for publishing and is scheduled for deployment in the Fall of 2025. An educational video miniseries is also in the works for IPHA-TV and is produced by AngioMedical Media. Both projects showcase a documentary tour of Phil Muccio's work leading to the development of his groundbreaking innovation.
At the same time, my experience with clubfoot meant I had to navigate the medical system firsthand. I was no stranger to hospital stays, leg casts, and the process of rehabilitation. These interactions shaped me deeply, instilling a sense of awe and respect for the doctors who helped me walk. But more than that, it made me acutely aware of the limitations in assistive technologies and rehabilitation methods available to patients. I knew I wanted to do something to improve this field.

I was a relentless tinkerer. Working from my basement, I built prototype after prototype, refining the design with each iteration. The goal was to create a solution that could be easily used at home, without the complexity and inconvenience of existing systems.

At the time, insurance companies had rigid standards for what they considered “acceptable” rehabilitation techniques. Electrical stimulation wasn’t widely embraced, and I found myself constantly fighting for recognition of its benefits. Many of my patients, particularly those with chronic pain, had been dismissed by the medical system—labeled as malingerers or hopeless cases. I refused to accept that. I saw time and again how my technology transformed lives, reducing pain, restoring mobility, and improving quality of life in ways conventional treatments could not.
My work with chronic pain patients further solidified my belief in the power of neuroprosthetics. Many individuals who had suffered for years, relying on ineffective pain management strategies, found relief through my technology. This reinforced my determination to continue developing and refining solutions despite institutional pushback.

The time for change is now. With the convergence of technology, healthcare innovation, and growing patient advocacy, I believe that neuroprosthetics will redefine rehabilitation. My journey, though marked by challenges, has always been guided by the belief that movement is fundamental to human dignity. Through persistence, innovation, and an unwavering commitment to patient care, I am determined to reshape the future of rehabilitation, ensuring that no one is left behind due to outdated methodologies or bureaucratic resistance.
However, I know I cannot do this alone. The future of neuroprosthetics requires a team—a collective of engineers, medical professionals, and visionaries who believe in this mission as much as I do. My journey has been long and at times exhausting, but I am not ready to stop. The lives of thousands, if not millions, of patients depend on the work we do today. And I am ready to see this revolution through.
IMPROVING QUALITY OF LIFE:
Axiobionics Arm BioSleeve helps a US Veteran regain arm function after a brain injury. Sgt. Shannon Mcallister was injured in an IED blast in Iraq causing a traumatic brain injury and left side paralysis. For more than a year the arm remained frozen and lifeless until he began wearing the Axio BioSleeve muscle stimulation system. "Sgt. McCallister realized that this technology was going to offer him the hope that he was looking for. And so I convinced Sergeant McAllister to let me design a wearable therapy sleeve, what we call an upper extremity neural prosthesis. We targeted three muscle groups and I wanted to rebuild these muscles for him. So he would have improved upper extremity, strength and control and function. It didn't take very long for him to actually get to the point where he was using the arm again, functionally."
REPORT FOR DEVICE #1 APPLICATION ON BACK INJURY / PAIN
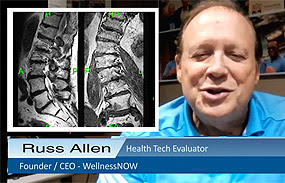
The injury incident happened on the 27th of January where I fell on my backside. I acquired the original MRI showing the fracture. Since the injury, the pain sensation was stable (not increasing or decreasing) for over six weeks prior to inducing the AxioBionics therapeutic device. I had a 12% compression fracture of the lumbar vertebra (which is a midline structure) where the pain was most evident on the left side. The sensation rating or pain level was consistent at 4 over 10. When I received the new Axiobionics neurostim unit on 3/4, received ample training from their tech consultant and I applied it directly on the pain on 3/5 for 20 minutes as part of my observational study. I also logged any physical reaction while maintaining the device's function setting of 4 and kept this setting throughout the review period.
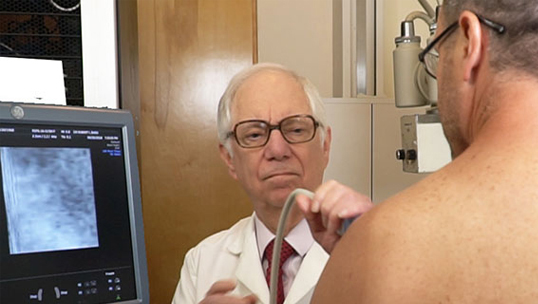
As part of exploring different scanning options, I used two different ultrasound probes; the linear probe at 18 mHz and the curved probe at 14 mHz. The ultrasound transverse (which means it's from right to left across the spine) shows the arrow pointing to the spinous process, which is the high point in the back that one can feel. The edematous area (labeled in yellow) shows it more to the left of midline as per the arrow.

ENDING STATEMENT: There is a different relationship between swollen tissue and the pain sensation. They often related temporally, but the compression of the pain fibers come from edematous pressure on the nerves. And if the nerves are relieved sufficiently, even though there's minimal healing or decrease in the tissue, the pain level may decrease significantly locally. After one week of repeated therapeutic application of the neurostim, the pain has been completely eliminated (0/10). The big takeaway from this experiment is the potential future where patients have their own therapeutic neurostim devices AND their own portable scanners to track their pain and injury. This allows them to know how to go forward.
Therapeutic Innovation for Arm Paralysis Interview by: Phil Muccio, CEO/AxioBionics  A recent patient (Kyle) was being treated for left sided hemiplegia. This entails trying to work with an arm that has been paralyzed by some event. The patient was experiencing unrelenting seizures that necessitated a procedure called a hemispherectomy. This surgical procedure will result in the paralysis of the opposite side of the body. He does a trade-off of course, because you can't live your life with unrelenting seizures. Through this process, if the motor cortex is involved, it's going to leave the opposite side of your body paralyzed. But in Kyle's case, he has some brain control so we wanted to help improve his functionality. (click image to see VIDEO) Instead of putting his arm in a sling, you want to do the exact opposite to encourage muscle activity and the connection between the brain and the muscles. The patient needs to condition this arm in a manner that he isn't able to do so, but in addition to this, you want to diminish the known problems of paralysis, which are muscle spasms, joint, stiffness, contractures. In a sling, the hand may clench and the elbow may flex- but it kind of leaves you with a clipped wing in a sense-- it's very difficult to use an arm like that. Through NEUROPROSTHETICS, we found a way to put muscle activity back into a paralyzed arm by placing our electric stimulation sleeves on his arm- enabling the patient to access muscle therapy daily, and that arm is active the entire time. It is making the muscles move contract and otherwise be very active, and in that process, we're helping to increase the connection between the brain and the muscle that's called MUSCLE RE-EDUCATION. And if you can lower the muscle spasms that tend to restrict movement, then that patient's arm will be easier to move. If you're locked up by muscle tightness, even small amounts of brain control will be rendered because you can't move against the restrictions of muscle spasms. It's important for us to alleviate those spasms to allow the brain to start using the muscles more effectively. * Check out additional stories like this from AXIOBIONICS.com |
Restoring Quality of Life with Ultrasound Studies and NeuroProsthetics
"CRIME SCENE" - From an interview with Dr. Robert L. Bard
Ultrasound uses Doppler blood flow sonography that measures vascular activity that is elevated in inflammatory states. The image showed four times the normal vessels supplying a non inflamed joint and the 3D/4D quantitative image of the hemodynamic activity confirmed moderate neovascularity in the region. This type of inflammation is also called “inflammatory spondylitis” originally described in the radiology journals and rheumatology literature in 2010. This is a critical distinction categorized under the heading of “arteritis” which is a diffuse disorder also affecting the blood vessels including the brain arteries and eye vasculature resembling Rheumatoid Arthritis in progressive clinical course. The 2021 International Inflammatory Skin Conference at the New York Academy of Medicine made the connection of inflammatory disease to heart disease and stroke and also to increased cancer risk. For example, the common skin disease psoriasis of the nail often develops into painful joint swelling and tendinitis. Rosacea of the nose is associated with inflammation of the eye. Gout with a painful toe may foreshadow the beginning of kidney disease or due to the body’s reaction to a high blood pressure medicine.

Ultrasound is non invasive, portable in some cases, real time and shows functional changes as far as abnormal structure (bone fracture vs sprain) and altered hemodynamic such as cancer vessels supplying an aggressive melanoma or breast cancer. Dynamic sonography of the joints is available without an MRI scanner and microcalcium (gout crystals) are visible in seconds that are invisible to most xrays and MRI scans (calcium stones appear black on MRI while showing bright white on sonograms. Point of care ultrasound (POCUS) is now used by the military to bring the diagnostics to the injured patient and at home use of this technology monitors COVID-19 patients avoiding hospitalization.
 |
| Russ Allen (R) "reclaiming the best of life" with family in active travels and sports |
 The imaging that I've used to diagnose my conditions included ultrasound, MRI, and an x-ray, all of which give different insight into what's going on in my body. The benefits of the ultrasound are I'm able to see inflammation within the nerves and muscles of my body. These would not be apparent in the MRI or an x-ray in the same way. The x-ray was able to dramatically show the curvature of my body. And the MRI is able to see the degradation of the ver vertebra in my back. The ultrasound is used on the most sensitive tissues in the most sensitive areas (including little babies inside their mothers).
The imaging that I've used to diagnose my conditions included ultrasound, MRI, and an x-ray, all of which give different insight into what's going on in my body. The benefits of the ultrasound are I'm able to see inflammation within the nerves and muscles of my body. These would not be apparent in the MRI or an x-ray in the same way. The x-ray was able to dramatically show the curvature of my body. And the MRI is able to see the degradation of the ver vertebra in my back. The ultrasound is used on the most sensitive tissues in the most sensitive areas (including little babies inside their mothers).
Leadership in the medical community is comprised of an array of difference makers. Many have committed to the noble profession of providing direct patient care while others dedicate their lives to research and exploration. And then there is that special breed of visionary whose best work is in pioneering new ground as technical innovators - reinventing the very future of protocols and clinical strategies. It is this type of healer that holds the unique ability to see beyond the current trends with the creative courage to risk, explore and pave new ventures.
Recent decades have abundantly shown the synergy between technology and medicine, together blazing new trails of problem solving for the human need to heal, recover and restore quality of life- all in the name of life extension. "In the case of Russ Allen, quality of life with chronic pain is greatly affected and it limits the ability to perform normal activities of daily living.



{kind=link}