
By Dr. Robert L. Bard

According to the Society for Women's Health Research, Over 20,000 women will be diagnosed with ovarian cancer this year in the United States and women have a 92% chance of surviving for five years post-diagnosis. However, more than three-fourths of women are not diagnosed until later stages." [2] Abnormal ovaries are often benign simple cysts, however the complex cysts are classifiable with the new ultrasound scoring system as to how suspicious they may be. The same way we detect prostate tumors by routine yearly ultrasound screening in high risk patients, we could save many lives because sometimes the first sign of ovarian cancer is a gland in the neck that pops up, a mass under the arm or jaundice because the liver is filled with metastatic tumor.

(1)-Hassani/Bard Gynecologic Ultrasound SpringerHeidelberg 1978 (2)-"Ovarian Cancer: Outdated Diagnostics for a Deadly Disease" Society for Women's Health Research 2020. https://swhr.org/ovarian-cancer-outdated-diagnostics-for-a-deadly-disease/ (3)-Awad M etal PEMF in Primary Dysmenorrhea 2020 MJCU 88;2165-2175 (4)-Thabet A etal High intensity Laser vs PEMF in Dysmenorrhea J Phys Ther Sci 2017 10:1742-1748
Uterine Fibroids: New Approaches to an Underdiagnosed Health Issue
Written and produced by: Dr. Roberta Kline for the Women's Health Digest / Balance & Longevity educational seminar series.
 |
FIBROIDS are the most common tumor of the female pelvis and are the number one reason for hysterectomy. While prevalence estimates vary widely, in part due to systemic underdiagnosis, they range worldwide from 4-70%. Globally, Black women have the highest rate, often 3x that of White women. In addition, Black women are more likely to have more severe symptoms and undergo hysterectomy at an earlier age, adding the burden of lost fertility for these women. The economic burden is also enormous. It is estimated that fibroids contribute to up to $34 billion in direct and indirect healthcare costs every year. [1]
WHAT ARE FIBROIDS?
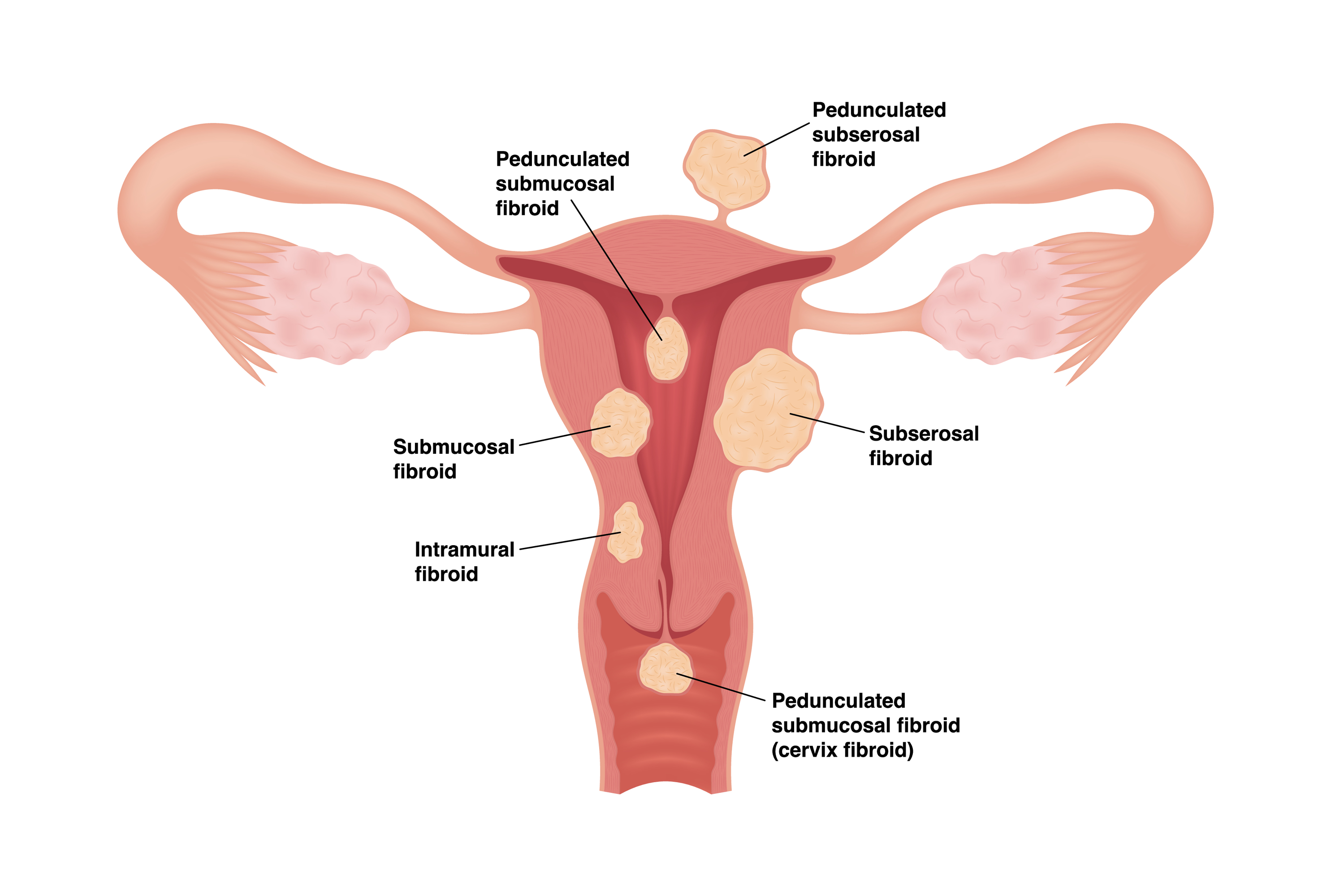 |
| Fibroids are classified based on where they occur in the uterus. |
Uterine fibroids, also known as uterine leiomyomas, are benign growths within the uterine wall that are made up of the same smooth muscle tissue as normal myometrium. But for reasons that are still not fully understood, they form into 3-dimensional spheres rather than the linear, elongated pattern of normal tissue.
Up to half of all women with fibroids are symptomatic. Although fibroids are typically benign, they can cause significant health effects. The most common symptoms are painful periods and heavy menstrual bleeding. Pelvic pressure and pain during intercourse are not uncommon. Depending on their size and location, fibroids can press on nerves and cause pain; obstruct nearby organs including ureters, bladder, and intestines. Fibroids can also cause reproductive problems including infertility, recurrent pregnancy loss, and other complications of pregnancy.
Genetics clearly plays a role. Having a family member with fibroids increases the risk – and if it’s your mother, you are 3x more likely to develop them too. A hereditary mutation in the FH gene (fumarate hydratase) that causes renal cell carcinoma (HRCC) is now being linked to the development of fibroids, especially at younger ages. [3]
One of the surprising findings of gene expression research is that almost half of all fibroids have chromosomal abnormalities. [5] Despite this, progression to the cancerous form (leiomyosarcoma) is rare – less than 1%. As researchers look deeper, it appears that it is not the genetic changes within the fibroid that have the most influence on the development of fibroids and the progression to cancer. Rather, it is the microenvironment, or the cellular health around the fibroid, that has this role. [6]
Therefore, it may be that improving the microenvironment in which these fibroids develop could be effective early intervention strategies. Noninvasive therapies that can reduce inflammation and oxidative stress including diet, medication, PEMF, and photobiomodulation may be new opportunities for early intervention for fibroids as well. [7]
While genetic expression research on fibroids is shedding light on some of the genomic and genetic alterations that contribute to discrepancies between women of different ethnicities, it is clear that these aren’t the only drivers. [8] As with many other health conditions, where a woman lives and works plays an outsized role.

Environmental toxins including endocrine disruptors and air pollution, stress, and socioeconomic status all have been shown to be connected with higher rates of fibroids. These are likely related to bidirectional effects of epigenetic alterations, access to care and bias within the healthcare system, as well as other factors still to be identified. [9]

Image source: Freytag, D., Günther, V., Maass, N., & Alkatout, I. (2021). Uterine Fibroids and Infertility. Diagnostics, 11(8). https://doi.org/10.3390/diagnostics11081455 [OPEN ACCESS}

Current treatment options include medication to address symptoms – accounting for up to 70% of women at some point. Surgery to remove the fibroids (myomectomy) or the entire uterus along with the fibroids (hysterectomy) is the oldest and most invasive option. Newer techniques such as laparoscopy have improved these surgical approaches. Within the past couple of decades uterine artery embolization (UAE) has offered a less invasive option, and newer noninvasive approaches are now emerging that utilize radiofrequency ablation (RFA), and high intensity focused ultrasound (HIFU). [2]
Here, too, treatment options are impacted by ethnicity and socioeconomic factors. "Despite minimally invasive options, Black women continue to dominate the percentages of women having hysterectomies for benign disease," Marsh says. "We need to understand why." [1]
One of the main limitations for these newer techniques is that they are more effective on smaller fibroids. Since fibroids tend to grow over time, it would seem a benefit to have earlier diagnosis so that women have better treatment options. In fact, a recent study in Ghana showed that routine ultrasounds at yearly clinic visits increased the rate of diagnosis, and at younger ages. [10]
REFERENCES
(1) Marsh, E. E., Al-Hendy, A., Kappus, D., et al. (2018). Burden, Prevalence, and Treatment of Uterine Fibroids: A Survey of U.S. Women. Journal of Women's Health, 27(11), 1359-1367. https://doi.org/10.1089/jwh.2018.7076 (2) Freytag, D., Günther, V., Maass, N., & Alkatout, I. (2021). Uterine Fibroids and Infertility. Diagnostics, 11(8). https://doi.org/10.3390/diagnostics11081455 (3) Lu, E., Hatchell, K. E., Nielsen, S. M., et al. (2022). Fumarate hydratase variant prevalence and manifestations among individuals receiving germline testing. Cancer, 128(4), 675-684. https://doi.org/10.1002/cncr.33997 (4) Välimäki N, Kuisma H, Oskari AP et al. (2018) Genetic predisposition to uterine leiomyoma is determined by loci for genitourinary development and genome stability eLife 7:e37110. (5) Kubínová K, Mára M, Horák P, et al. Genetic factors in etiology of uterine fibroids. Ceska Gynekol. 2012 Feb;77(1):58-60. Czech. PMID: 22536642. (6) Bharambe, B. M., Deshpande, K. A., Surase, S. G., & Ajmera, A. P. (2014). Malignant Transformation of Leiomyoma of Uterus to Leiomyosarcoma with Metastasis to Ovary. Journal of Obstetrics and Gynaecology of India, 64(1), 68-69. https://doi.org/10.1007/s13224-012-0202-4 (7) Tinelli, A., Vinciguerra, M., Malvasi, A., et al. (2021). Uterine Fibroids and Diet. International Journal of Environmental Research and Public Health, 18(3), 1066. https://doi.org/10.3390/ijerph18031066 (8) Edwards, T. L., Giri, A., Hellwege, J. N., et al. (2019). A Trans-Ethnic Genome-Wide Association Study of Uterine Fibroids. Frontiers in Genetics, 10. https://doi.org/10.3389/fgene.2019.00511 (9) Cheng, L., Li, H., Gong, Q., et al. (2022). Global, regional, and national burden of uterine fibroids in the last 30 years: Estimates from the 1990 to 2019 Global Burden of Disease Study. Frontiers in Medicine, 9, 1003605. https://doi.org/10.3389/fmed.2022.1003605 (10) Mesi Edzie, E. K., Dzefi-Tettey, K., Brakohiapa, E. K., et al. (2023). Age of first diagnosis and incidence rate of uterine fibroids in Ghana. A retrospective cohort study. PLOS ONE, 18(3), e0283201. https://doi.org/10.1371/journal.pone.0283201
ABOUT THE AUTHOR

ROBERTA KLINE, MD (Educational Dir. /Women's Diagnostic Group) is a board-certified ObGyn physician, Integrative Personalized Medicine expert, consultant, author, and educator whose mission is to change how we approach health and deliver healthcare. She helped to create the Integrative & Functional Medicine program for a family practice residency, has consulted with Sodexo to implement the first personalized nutrition menu for healthcare facilities, and serves as Education Director for several organizations including the Women’s Diagnostic Health Network, Mommies on a Mission. Learn more at https://robertaklinemd.com/

Copyright Notice: The materials provided on this newsletter article is copyrighted and is the intellectual property of Dr. Roberta Kline as the writer/producer and or publisher. It is also under the protection of the (Integrative Cancer Resource Society and the AngioFoundation(201c3). This feature report is published strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site (BALANCE & LONGEVITY) and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.


